Malignant glaucoma was originally identified in 1869 as having an increased IOP and a shallow or flat anterior chamber, typically following ocular surgery. Aqueous misdirection, ciliary block glaucoma, and lens block angle closure are some of the many terms for malignant glaucoma that have evolved through time. It is one of the most complex and challenging glaucoma to cure, and if left untreated, it can possibly lead to total blindness.
The main signs and symptoms of malignant glaucoma are bleb needling, infection and inflammation, retinal detachment, retinopathy of prematurity, and trauma.
Prior angle closure glaucoma, trabeculectomy filtration surgery, peripheral laser iridotomy, cyclophotocoagulation, and use of miotics are the causes of malignant glaucoma.
Typically, 2 to 4 percent of eyes that receive surgery for angle closure glaucoma develop malignant glaucoma.
Although it can happen at any time after the procedure, incisional surgery is the most common time for it to happen. A trabeculectomy or cataract extraction with or without IOL (intra ocular lens) implantation are examples of iatrogenic reasons that might lead to this condition.
Prior to surgery, every attempt should be taken to stop an attack if angle glaucoma is present.
Mydriatic cycloplegic therapy should be started after iridotomy and prolonged indefinitely if the attack cannot be stopped.
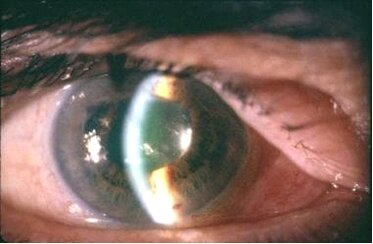
Malignant glaucoma is challenging to diagnose and treat. In phakic and pseudophakic individuals, the slit-lamp examination will show the anterior displacement of the lens-iris diaphragm. Physical signs of malignant glaucoma include uneven anterior chamber depths, growing myopia, and progressive anterior chamber shallowing. If the patency of the iridectomy is in doubt a laser iridotomy can be performed again to exclude pupil block. It is simple for doctors to determine that you have hypotony if they discover a shallow anterior chamber connected to a wound leak. Hypotony may be accompanied by choroidal effusion or excessive draining into the subconjunctival region if there is no wound leak. If the iridotomy is patent high, choroidal hemorrhage should be suspended either clinically or by ultrasound examination
Treatment for malignant glaucoma focuses on decreasing IOP with aqueous suppressants, narrowing the vitreous with hyperosmotic drugs, and trying to posteriorly displace the lens-iris diaphragm using a potent cycloplegic like atropine. If a laser iridotomy is required or if the patency of an existing iridotomy cannot be verified, either one should be carried out. Medical treatment has a delayed effect, but within five days, roughly 50% of instances of malignant glaucoma will be resolved.
If medical treatment is unsuccessful, YAG laser therapy may be used to disturb the posterior capsule and anterior hyaloid face. When laser therapy is not feasible or is unsuccessful, posterior vitrectomy must be performed with disruption of the anterior hyaloid face.
At The Eye Center- Dr. Mahnaz Naveed Shah & Associates our team of eight ophthalmology subspecialists/ eye specialists, eye surgeons who are considered amongst the very best eye specialists in Karachi and in Pakistan, have the diagnostic and treatment capabilities to treat from the simplest to the most complex patients. We work hard to provide our patients with the best possible medical and surgical eye care, in a state of the art purpose built eye care facility. We offer the entire array of medical, laser and surgical treatments to help provide patients the best possible care in the most efficient, safe and ethical manner.
If you need an appointment, please contact us at 03041119544 during our working hours or leave us a WhatsApp message at +923028291799 and someone will connect with you. Walk-in appointments are also available for emergencies. We can also be reached through our web portal on www.surgicaleyecenter.org